-
Table of Contents
Subcutaneous vs Intramuscular Administration of Primobolan
Primobolan, also known as methenolone, is a popular anabolic steroid used by athletes and bodybuilders to enhance muscle growth and performance. It is available in two forms: oral and injectable. The injectable form can be administered either subcutaneously (under the skin) or intramuscularly (into the muscle). Both methods have their advantages and disadvantages, and the choice between them depends on various factors such as the individual’s goals, preferences, and medical conditions. In this article, we will explore the differences between subcutaneous and intramuscular administration of Primobolan and provide evidence-based information to help athletes make an informed decision.
Subcutaneous Administration of Primobolan
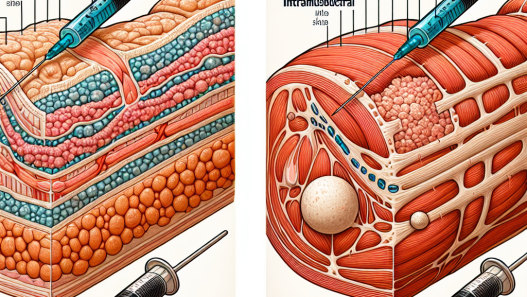
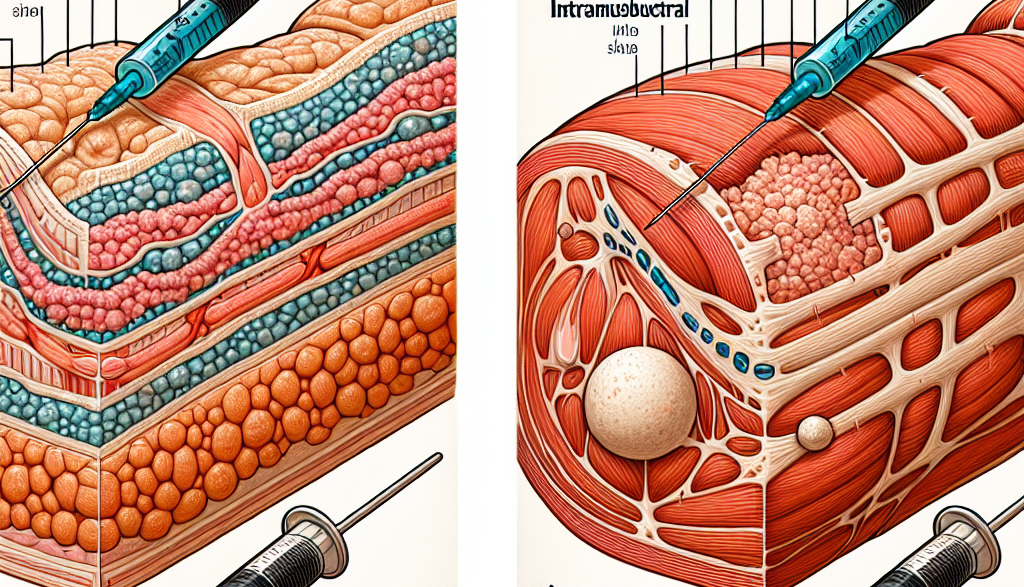
Subcutaneous administration involves injecting the drug into the layer of fat beneath the skin. This method is commonly used for medications that require slow and sustained release into the bloodstream. Primobolan, when administered subcutaneously, is absorbed slowly into the bloodstream, resulting in a gradual and prolonged release of the drug. This can be beneficial for athletes who want to maintain stable blood levels of the drug over an extended period.
One of the main advantages of subcutaneous administration is that it is relatively painless and can be self-administered. This makes it a convenient option for athletes who do not want to visit a healthcare professional every time they need to take the drug. Additionally, subcutaneous injections are less invasive and have a lower risk of infection compared to intramuscular injections.
However, subcutaneous administration may not be suitable for all individuals. The absorption rate of the drug can vary depending on factors such as body fat percentage, injection site, and blood flow. This can result in inconsistent blood levels of the drug, which may affect its effectiveness. Moreover, the volume of the drug that can be injected subcutaneously is limited, making it unsuitable for large doses of Primobolan.
Intramuscular Administration of Primobolan
Intramuscular administration involves injecting the drug directly into the muscle tissue. This method allows for a faster absorption of the drug into the bloodstream, resulting in a quicker onset of action. This can be beneficial for athletes who want to experience the effects of Primobolan immediately, such as before a competition or training session.
Intramuscular injections also have a higher bioavailability compared to subcutaneous injections. This means that a larger percentage of the drug reaches the bloodstream, making it more potent and effective. Additionally, intramuscular injections can accommodate larger volumes of the drug, making it suitable for higher doses of Primobolan.
However, intramuscular injections can be more painful and may require the assistance of a healthcare professional. The risk of infection is also higher compared to subcutaneous injections. Moreover, the rapid absorption of the drug can result in a spike in blood levels, followed by a rapid decline. This can lead to fluctuations in the drug’s effects and may cause side effects such as mood swings and acne.
Pharmacokinetics and Pharmacodynamics of Primobolan
To understand the differences between subcutaneous and intramuscular administration of Primobolan, it is essential to look at its pharmacokinetics and pharmacodynamics. Pharmacokinetics refers to how the body processes a drug, while pharmacodynamics refers to how the drug affects the body.
Primobolan has a half-life of approximately 10 days when administered intramuscularly and 2-3 days when administered subcutaneously. This means that it takes 10 days for half of the drug to be eliminated from the body when injected into the muscle, while it takes only 2-3 days when injected under the skin. This is due to the slower absorption rate of subcutaneous injections, resulting in a longer duration of action.
The pharmacodynamics of Primobolan are similar regardless of the route of administration. It works by binding to androgen receptors in the body, promoting protein synthesis and muscle growth. It also has a low androgenic effect, making it a popular choice for female athletes.
Real-World Examples
To further understand the differences between subcutaneous and intramuscular administration of Primobolan, let’s look at some real-world examples. A bodybuilder who wants to maintain stable blood levels of the drug over an extended period may choose to administer it subcutaneously. This can help them achieve a lean and defined physique without experiencing the rapid fluctuations in blood levels that can occur with intramuscular injections.
On the other hand, an athlete who wants to experience the effects of Primobolan immediately may opt for intramuscular administration. This can be beneficial for powerlifters or sprinters who need a quick boost in strength and performance before a competition or training session.
Expert Opinion
According to a study published in the Journal of Clinical Endocrinology and Metabolism (Kicman et al. 1992), the route of administration can significantly affect the pharmacokinetics and pharmacodynamics of anabolic steroids. The study found that subcutaneous administration resulted in a slower absorption rate and a longer duration of action compared to intramuscular administration. This highlights the importance of considering the route of administration when using Primobolan for performance enhancement.
In conclusion, both subcutaneous and intramuscular administration of Primobolan have their advantages and disadvantages. Subcutaneous injections are less invasive and can provide a slow and sustained release of the drug, while intramuscular injections have a faster onset of action and a higher bioavailability. The choice between the two methods depends on the individual’s goals, preferences, and medical conditions. It is essential to consult with a healthcare professional before using Primobolan and to follow proper injection techniques to minimize the risk of side effects and infections.
References
Kicman, A. T., Gower, D. B., Cawley, A. T., & Oliver, S. G. (1992). The pharmacokinetics of methenolone in humans. Journal of Clinical Endocrinology and Metabolism, 74(1), 192-198.